POR QUÉ IMPORTA
El COA es el documento que separa los biológicos reales del marketing
Los productos de exosomas están apareciendo en medspas, consultorios de dermatología, clínicas de restauración capilar y ensayos clínicos dermatológicos a un ritmo que supera la claridad regulatoria de la categoría. Algunos de esos productos están genuinamente bien caracterizados. Otros llegan con un folleto llamativo, una referencia vaga a la “tecnología de células madre” y un documento de una página que se autodenomina Certificado de Análisis pero que se lee más como una ficha de marketing.
Para un profesional con licencia, el Certificado de Análisis es el documento más importante de la relación con el proveedor. Es lo que permite a un clínico defender una decisión de tratamiento en una nota de historia clínica, en una revisión por pares, ante una junta médica estatal y ante un paciente que merece saber qué se le está aplicando. Leer un COA como lo lee un químico, revisando los ensayos, las unidades, los métodos y los controles negativos, es una competencia esencial del profesional en esta categoría.
Este artículo recorre la ciencia: qué marcadores de superficie porta un exosoma real, qué microARN realizan el trabajo biológico, qué fuentes de célula estromal mesenquimal (MSC) producen qué perfiles de carga y qué criterios de valoración de ensayos clínicos están empezando a traducir la señal preclínica en resultados medibles. Luego recorre el propio COA, parámetro por parámetro, con el marco analítico que MISEV 2023 ha codificado para el campo.
| Rango de tamaño de exosoma de 30 a 150 nm | ≥ 3 marcadores Mínimo MISEV 2023 (CD9, CD63, CD81) | < 5 EU/kg/h Límite de endotoxina estándar, USP <85> |
LA BIOLOGÍA
Qué es realmente un exosoma
Un exosoma es una vesícula extracelular pequeña, de entre 30 y 150 nanómetros de diámetro, formada dentro de la célula parental a través de la vía endosomal. Los endosomas tardíos maduran en cuerpos multivesiculares (MVB), que contienen vesículas intraluminales. Cuando un MVB se fusiona con la membrana plasmática, esas vesículas intraluminales se liberan al espacio extracelular como exosomas. Esta vía de biogénesis los distingue de las microvesículas, que brotan directamente de la membrana plasmática, y de los cuerpos apoptóticos, que se liberan durante la muerte celular [1].
El interés terapéutico en los exosomas es inseparable de su carga. Cada vesícula transporta una mezcla compleja de proteínas, lípidos, ARNm y microARN que refleja la biología de la célula parental. Cuando un exosoma alcanza una célula receptora mediante fusión, unión a receptor o endocitosis, entrega un mensaje biológico de múltiples vías. Una revisión de 2024 en Signal Transduction and Targeted Therapy describe a los exosomas como herederos de los efectos terapéuticos de sus células parentales a través de esta entrega, evitando a la vez los riesgos asociados a la administración de células vivas [1].
Para los profesionales, tres categorías de biología merecen atención antes de leer cualquier COA: los marcadores de superficie que confirman la identidad del exosoma, la carga de microARN que impulsa el efecto biológico posterior y la fuente celular parental que determina, en primer lugar, cómo es esa carga.
MARCADORES DE SUPERFICIE
La tríada de tetraspaninas: CD9, CD63 y CD81
Tres tetraspaninas, CD9, CD63 y CD81, son los marcadores de superficie canónicos que se usan para identificar exosomas. Pertenecen a una familia de proteínas de cuatro dominios transmembrana que organiza microdominios de membrana llamados microdominios enriquecidos en tetraspaninas (TEM). Cada una de las tres cumple funciones biológicas distintas en la célula parental, ocupa compartimentos subcelulares diferentes y contribuye de forma distinta al comportamiento de la vesícula [2].
Figura 1. El marco MISEV 2023 para la identificación de exosomas requiere al menos tres marcadores positivos y un marcador negativo. CD9, CD63 y CD81 son la tríada canónica de tetraspaninas.
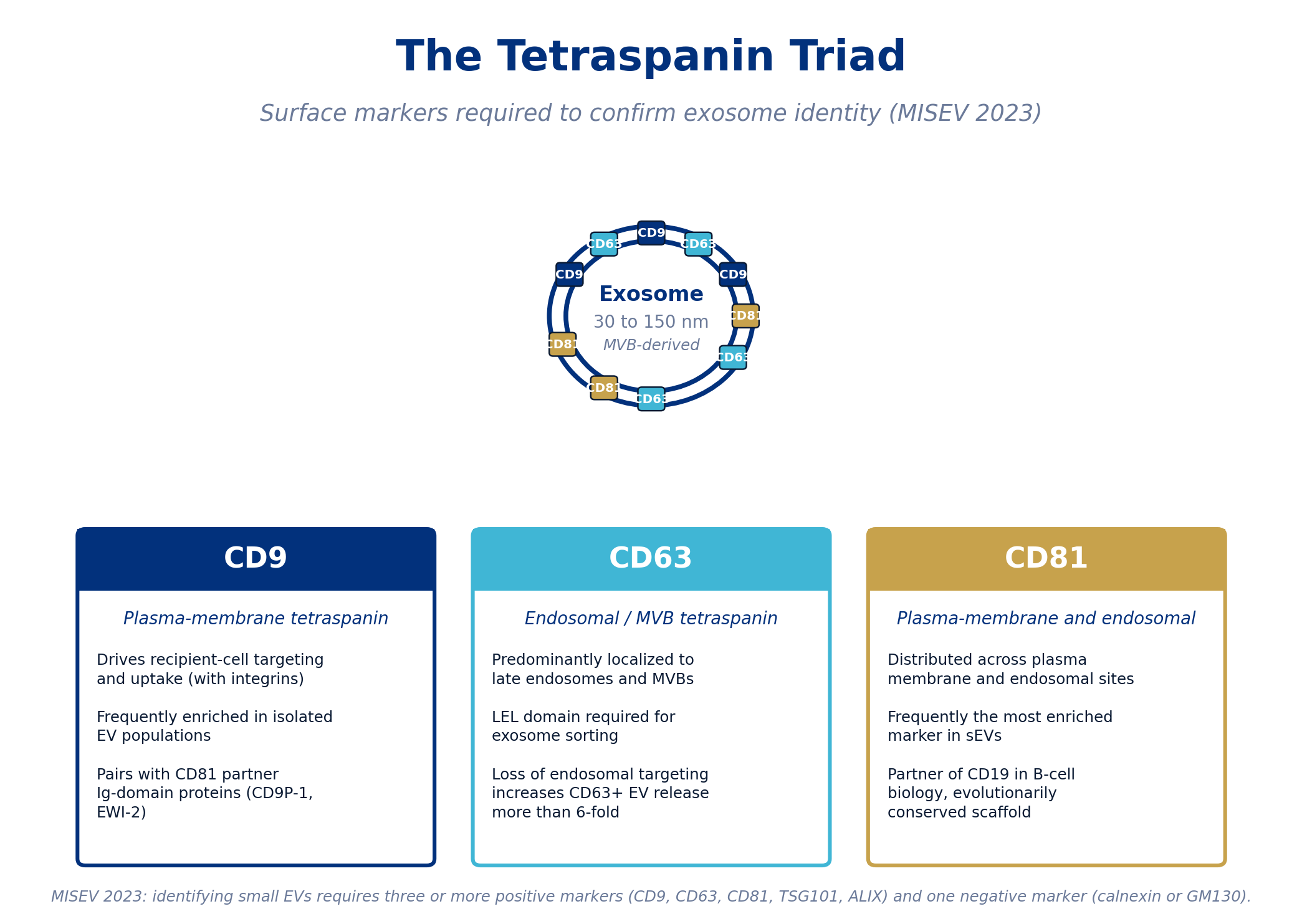
CD9: tetraspanina de la membrana plasmática que dirige la captación por la célula receptora
CD9 se localiza predominantemente en la membrana plasmática de la célula productora y aparece en la superficie de los exosomas secretados. Su función biológica está estrechamente ligada a la orientación y captación por la célula receptora. Se ha demostrado que CD9, junto con la integrina αvβ3, media la orientación de los exosomas hacia las células dendríticas [2]. CD9 se asocia con frecuencia con proteínas socias con dominio Ig, incluidas CD9P-1 y EWI-2, que cosegregan en las VE y pueden participar en la adhesión celular y la señalización [3]. Funcionalmente, las vesículas positivas para CD9 están enriquecidas en muchas preparaciones aisladas de VE, y CD9 es uno de los marcadores positivos que se detectan de forma más fiable en las distintas fuentes de MSC.
CD63: el marcador endosomal que define el origen del exosoma
CD63 es la tetraspanina más estrechamente asociada al compartimento endosomal. En las células productoras, CD63 se confina principalmente a los cuerpos multivesiculares, que es exactamente el compartimento donde se forman los exosomas [2]. El gran bucle extracelular (LEL) de CD63 porta una señal de clasificación crítica: cuando se elimina el LEL, CD63 no logra localizarse en los exosomas [4]. A la inversa, las modificaciones en el extremo C-terminal que alteran la orientación endosomal hacen que CD63 se reubique en la membrana plasmática y producen un aumento de más de seis veces en la liberación de VE positivas para CD63 [3]. Más allá de su papel como marcador, CD63 participa en la clasificación de la carga (un estudio de 2014 identificó una orientación de VE dependiente de CD63 en células de neuroblastoma [2]) y, a través de su complejo con la sintenina-1, en el tráfico de ciertas proteínas virales [3].
CD81: el marcador más enriquecido, con un papel conservado de andamiaje
CD81 se distribuye tanto en la membrana plasmática como en los compartimentos endosomales, y con frecuencia es la más enriquecida de las tres tetraspaninas en las preparaciones aisladas de VE pequeñas [3]. CD81 desempeña funciones bien caracterizadas fuera del campo de las VE, incluida su asociación con CD19 en la coestimulación de linfocitos B. Los ratones y humanos deficientes en CD81 muestran una inmunidad humoral deteriorada por la disminución de la expresión de CD19 [3]. En el contexto de las VE, CD81 forma un complejo de andamiaje con las mismas proteínas con dominio Ig (EWI-F y EWI-2) que se asocian con CD9, y la pérdida simultánea de CD9 y CD81 provoca una disminución medible de estas proteínas socias en las VE.
Mínimo de MISEV 2023: la identificación de vesículas extracelulares pequeñas requiere al menos tres marcadores positivos, tomados de las tetraspaninas (CD9, CD63, CD81) más candidatos opcionales como TSG101 o ALIX, junto con al menos un marcador negativo (calnexina, GM130 u otra proteína no vesicular) para confirmar la baja contaminación por restos celulares [5]. Un COA que reporta una sola tetraspanina no cumple este mínimo.
BIOLOGÍA DE LA CARGA
Carga de microARN: el extremo funcional de la terapia
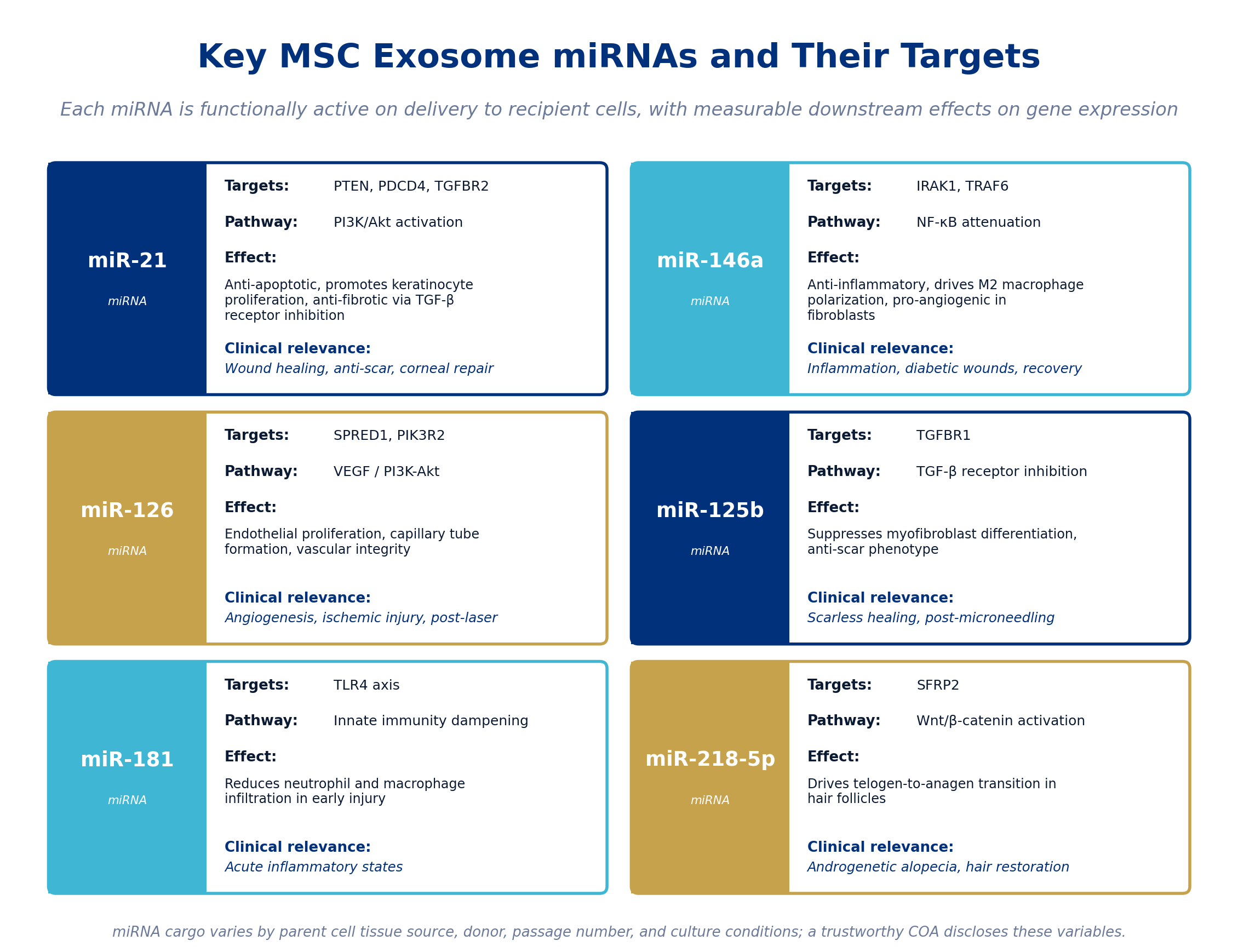
Los marcadores de superficie confirman qué es un exosoma. Los microARN explican qué hace un exosoma. Una revisión de 2024 de exosomas derivados de MSC describe su carga de microARN como un repertorio reproducible y específico del tipo celular que entrega efectos posteriores medibles sobre la expresión génica una vez internalizado por las células receptoras. Los microARN no actúan de forma independiente; se agrupan en torno a un pequeño número de vías (PI3K/Akt, NF-κB, TGF-β/SMAD, VEGF, Wnt/β-catenina) que, en conjunto, explican la mayor parte de la biología regenerativa descrita en la literatura.
Figura 2. Seis de los microARN más estudiados en los exosomas de MSC, con sus dianas directas, vías de señalización, efectos biológicos y relevancia clínica.
miR-21: antiapoptótico y antifibrótico
miR-21 es uno de los microARN más abundantes en los exosomas derivados de MSC y está sobreexpresado en los exosomas de MSC de cordón umbilical humano junto con miR-146a y miR-181 [6]. Sus dianas principales son PTEN y PDCD4, ambos reguladores negativos de la vía PI3K/Akt. Al suprimirlos, miR-21 promueve la supervivencia, la proliferación y la migración celular. En un estudio de 2022, las VE pequeñas de MSC de cordón umbilical humano aceleraron la cicatrización del epitelio corneal mediante la entrega de miR-21 y la activación del eje PTEN/PI3K/Akt [7]. miR-21 también actúa sobre TGFBR2: en un estudio de 2021 en Stem Cell Research and Therapy, los exosomas de MSC de sangre de cordón umbilical que portaban miR-21-5p y miR-125b-5p inhibieron la señalización del receptor de TGF-β, suprimieron la diferenciación de miofibroblastos y redujeron la formación de cicatrices en modelos de cicatrización [8]. La relevancia clínica se concentra en la proliferación de queratinocitos, la remodelación antifibrótica y las aplicaciones de cicatrización de heridas.
miR-146a: atenuación de NF-κB y polarización M2
miR-146a actúa sobre IRAK1 y TRAF6, dos proteínas adaptadoras de la cascada de señalización inflamatoria NF-κB. Al suprimirlas, miR-146a atenúa la producción de citocinas proinflamatorias y desplaza a los macrófagos hacia el fenotipo antiinflamatorio M2 [9]. En los exosomas de MSC, miR-146a es uno de los microARN responsables de la conversión de macrófagos de M1 a M2, junto con miR-9, miR-125b, miR-127 y miR-155 [9]. Un estudio de 2021 en Frontiers in Cell and Developmental Biology demostró que la senescencia inducida por peróxido de hidrógeno en las MSC reduce el contenido exosomal de miR-146a, y que esta pérdida deteriora sustancialmente la capacidad proangiogénica y procicatrizante de los exosomas resultantes [10]. El silenciamiento de miR-146a en exosomas frescos de MSC redujo su capacidad angiogénica, mientras que su sobreexpresión en exosomas de MSC senescentes rescató parcialmente el deterioro [10]. Los exosomas cargados con miR-146a mediante ingeniería han mostrado efectos antiinflamatorios y regenerativos pronunciados en modelos de cicatrización de heridas diabéticas [11]. miR-146a es la carga que hay que buscar en cualquier producto posicionado para inflamación, recuperación posprocedimiento o aplicaciones de heridas crónicas.
miR-126: el microARN proangiogénico específico del endotelio
miR-126 es el microARN específico del endotelio más directamente responsable de la integridad vascular y la angiogénesis. El trabajo original de 2008 de Wang y colaboradores en Developmental Cell identificó a miR-126 como regulador de la respuesta endotelial al VEGF, demostrando que miR-126 reprime dos reguladores negativos de la vía del VEGF: SPRED1 (una proteína relacionada con Sprouty) y PIK3R2 (la subunidad reguladora p85-β de PI3K) [12]. El silenciamiento de miR-126 en embriones de pez cebra produjo pérdida de la integridad vascular y hemorragia. En los exosomas de MSC, se ha demostrado que miR-126 acelera la angiogénesis en heridas de ratas diabéticas, y un estudio de 2021 en el Journal of Cellular and Molecular Medicine mostró que los exosomas de MSC de médula ósea que sobreexpresan miR-126 promovieron la proliferación, la migración y la formación de túbulos de las HUVEC mediante la activación de PI3K/Akt mediada por PIK3R2 [13]. Un estudio separado mostró que los exosomas derivados de MSC mejoran las células endoteliales lesionadas por hipoxia/reoxigenación al transferir miR-126 a través de la señalización PI3K/Akt/eNOS [14]. Para los profesionales de la medicina estética, miR-126 es la carga más directamente implicada en la revascularización posláser, posmicroagujas y posprocedimiento.
miR-125b y miR-181: moduladores anticicatriz y antiinflamatorios
miR-125b actúa sobre TGFBR1 y, junto con miR-21, contribuye a la supresión del eje TGF-β/SMAD que produce un fenotipo de cicatrización resistente a la cicatriz [8]. miR-181 amortigua la señalización de TLR4 y reduce el reclutamiento de neutrófilos y macrófagos en la lesión temprana, complementando el efecto de polarización de fase tardía de miR-146a [6]. Ambos microARN están sobreexpresados en los exosomas de MSC de cordón umbilical humano y contribuyen al perfil antiinflamatorio y de remodelación más amplio que distingue a los productos de MSC de cordón umbilical en la literatura.
miR-218-5p: el microARN de la restauración capilar
La biología de la papila dérmica del folículo piloso opera a través de la señalización Wnt/β-catenina, y miR-218-5p se sitúa de lleno en esa vía. Un estudio de 2020 en Science Advances demostró que miR-218-5p en los exosomas de células de la papila dérmica actúa sobre SFRP2, un inhibidor de la señalización Wnt, y que los miméticos de miR-218-5p promueven el desarrollo del folículo piloso mientras que los inhibidores bloquean la transición de telógeno a anágeno [15]. Una revisión sistemática de 2025 en tricología consolida el panorama más amplio: los exosomas derivados de MSC, ASC y DPC activan de forma consistente las vías Wnt/β-catenina, VEGF y PI3K/AKT e impulsan la transición de telógeno a anágeno, con datos clínicos preliminares prometedores en alopecia androgenética, alopecia areata y alopecia inducida por quimioterapia [16]. miR-218-5p es la carga más estrechamente ligada a los resultados de restauración capilar.
Conclusión para el profesional: si un proveedor no puede indicarle, en el COA o a pedido, qué fuente de tejido produjo los exosomas y cuál es el perfil dominante de microARN de su preparación, usted no tiene información suficiente para elegir el producto adecuado para su aplicación. La carga varía según la fuente de tejido, el donante, el número de pase y las condiciones de cultivo.
FUENTE CELULAR
La fuente importa: médula ósea, tejido adiposo y cordón umbilical
Las VE derivadas de MSC representan aproximadamente el 61 % de los estudios intervencionistas de VE registrados en ClinicalTrials.gov, pero “MSC” oculta una distinción biológica significativa. Un estudio proteómico de 2020 en Stem Cell Research and Therapy identificó 1.014 proteínas en exosomas derivados de MSC humanas de médula ósea, tejido adiposo y cordón umbilical, y encontró que, a pesar de funciones compartidas en las vías de receptores de la matriz extracelular, cada fuente tenía un énfasis funcional distinto [17].
Figura 3. Diferenciación funcional entre las tres fuentes dominantes de MSC usadas en la producción clínica de exosomas. La fuente determina la carga, y la carga determina la biología.
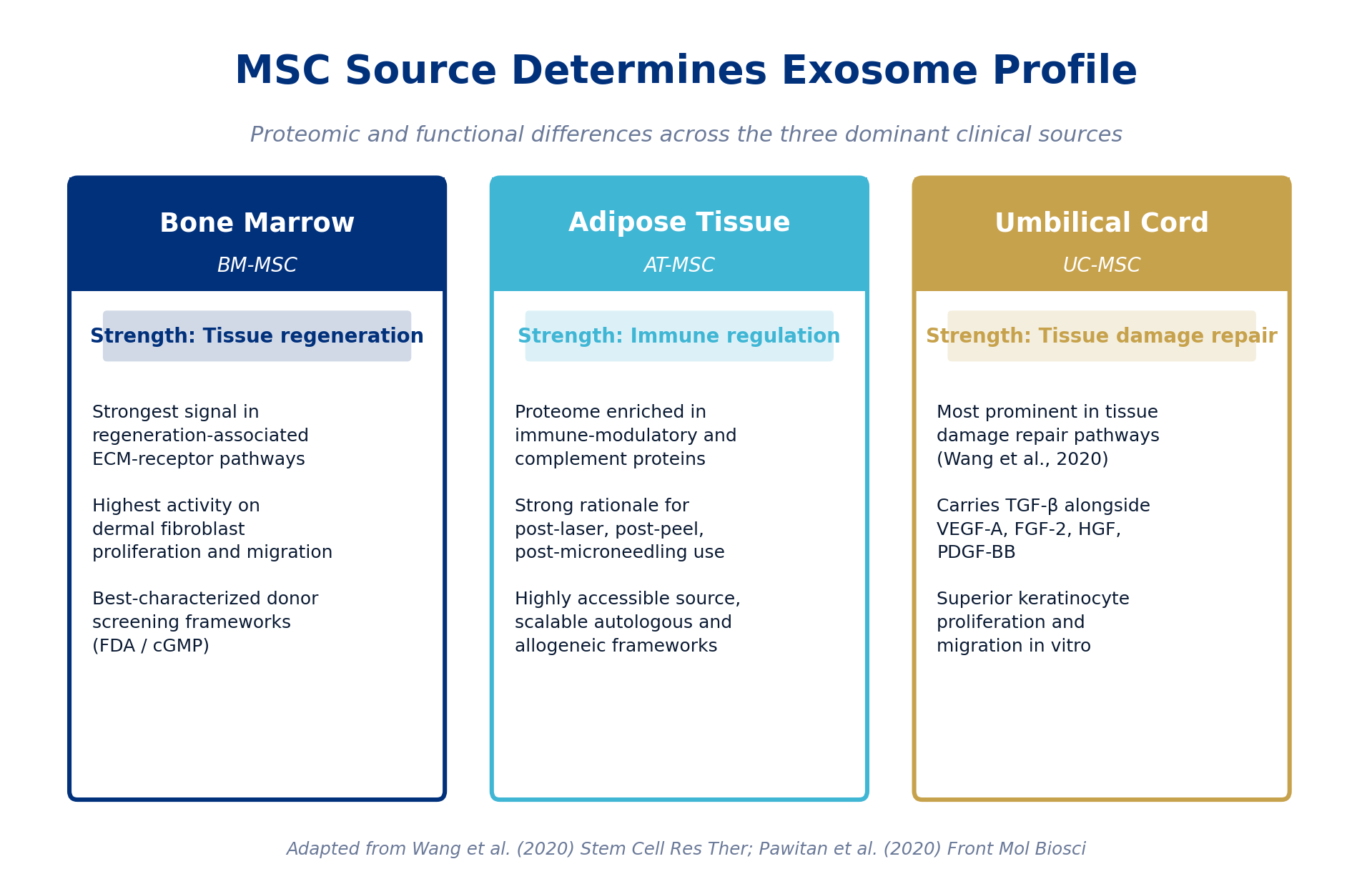
Los exosomas de MSC de médula ósea mostraron la señal más fuerte en las vías asociadas a la regeneración, y un estudio de cicatrización de 2020 en Frontiers in Molecular Biosciences confirmó que los exosomas de BM-MSC tenían la mayor actividad sobre la proliferación y migración de fibroblastos dérmicos en condiciones libres de suero [18]. Los exosomas de MSC de tejido adiposo estaban enriquecidos en proteínas inmunomoduladoras y de la vía del complemento [17], que es el perfil biológico que encaja con los casos de uso de recuperación posprocedimiento en medicina estética, como posláser, pospeeling y posmicroagujas. Los exosomas de MSC de cordón umbilical fueron los más prominentes en las vías de reparación del daño tisular [17] y fueron la única fuente que portaba TGF-β junto con VEGF-A, FGF-2, HGF y PDGF-BB; también mostraron una proliferación y migración de queratinocitos superior in vitro [18].
Una comparación proteómica de 2021 en el Iranian Biomedical Journal entre exosomas de UC-MSC y AD-MSC identificó 198 proteínas expresadas de forma diferencial y confirmó que los exosomas de UC-MSC están más fuertemente enriquecidos en vías inmunitarias, de activación del complemento y de cascada de activación de proteínas, mientras que las funciones compartidas se concentran en las cascadas de activación plaquetaria y coagulación [19]. Para los profesionales, la implicación práctica es directa: una afirmación genérica de “exosoma de MSC” no es suficiente. La fuente de tejido, la selección del donante y las condiciones de cultivo son variables de primer orden que afectan lo que una clínica está comprando realmente.
EVIDENCIA CLÍNICA
Lo que muestran los ensayos en aplicaciones estéticas y dermatológicas
El panorama de ensayos clínicos de exosomas en medicina estética y dermatología es real, está creciendo y se encuentra en su mayoría en Fase 1 y Fase 2. Una revisión de 2024 en Skin Health and Disease identificó cuatro ensayos clínicos prospectivos en rejuvenecimiento cutáneo. Park y colaboradores realizaron un estudio prospectivo, aleatorizado y de media cara con 28 sujetos que mostró que una preparación de exosomas derivados de MSC de tejido adiposo humano combinada con microagujas superó significativamente a las microagujas solas en la Escala Global de Mejoría Estética a las 6 semanas, con mejoras medidas en contenido de colágeno, reducción de arrugas, elasticidad, hidratación y despigmentación hasta las 12 semanas [20]. Proffer y colaboradores realizaron un ensayo de 56 participantes con un suero de exosomas derivados de plaquetas humanas de aplicación tópica y reportaron mejoras significativas en eritema, pigmentación y puntuación de arrugas a lo largo de 6 semanas [20].
Un ensayo de no inferioridad de media cara con evaluador cegado de 2025, publicado en el Journal of Cosmetic Dermatology, comparó exosomas derivados de MSC de tejido adiposo con plasma rico en plaquetas en el tratamiento con microagujas de radiofrecuencia para piel facial fotoenvejecida, la primera comparación directa de estas dos modalidades regenerativas en dermatología estética [21]. Una revisión sistemática de 2025 sobre ensayos clínicos de VE en el envejecimiento y la regeneración de la piel en el International Journal of Molecular Sciences sintetizó datos humanos y preclínicos de alta traslación hasta noviembre de 2024, caracterizando la categoría de exosomas derivados de plaquetas como una que muestra resultados estéticos consistentes y reproducibles en múltiples estudios [22].
En el lado de la restauración capilar, una revisión sistemática de 2025 en el World Journal of Stem Cells consolidó los argumentos a favor de los exosomas derivados de MSC en la alopecia androgenética, con mejoras en densidad y grosor del cabello respaldadas por la activación de la vía Wnt/β-catenina y un perfil de seguridad favorable en informes clínicos de cohortes pequeñas [23]. La revisión de 2024 en The Aesthetic Surgery Journal posicionó a los exosomas tópicos junto con los péptidos tópicos como las plataformas de biológicos acelulares que se desarrollan más activamente en dermatología, sin que ninguna esté aún aprobada por la FDA, pero con resultados preliminares medibles en múltiples criterios de valoración [24].
La base de evidencia es genuina, el mecanismo de acción está bien respaldado por la biología revisada por pares y la señal clínica temprana es consistente. Los ensayos de Fase 3 a gran escala, controlados con placebo, siguen siendo el siguiente punto de referencia.
DOCUMENTACIÓN DE CALIDAD
Cómo leer el COA: doce parámetros, en orden
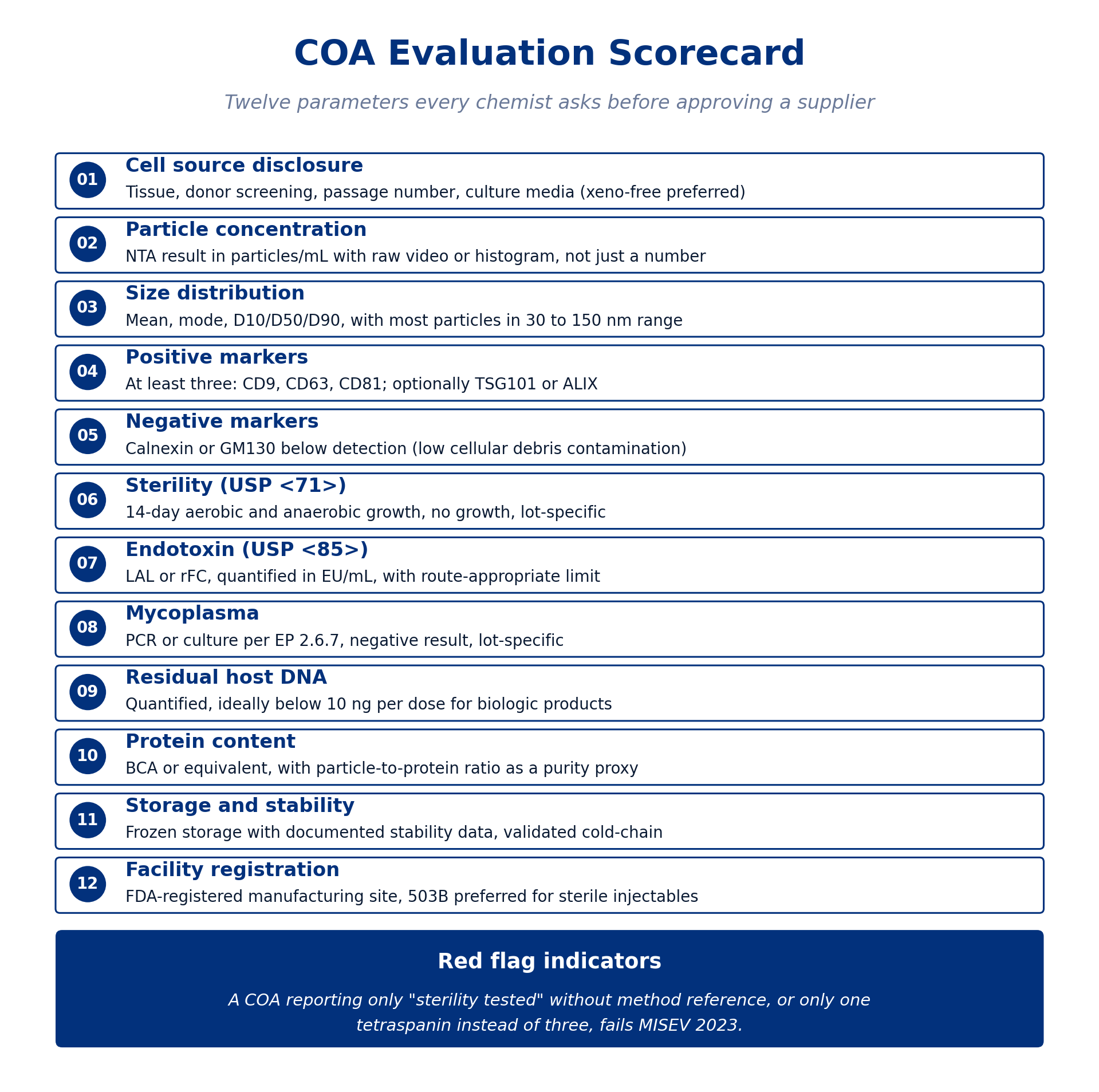
Un Certificado de Análisis es un documento estructurado. Leerlo correctamente significa saber qué categoría de información va en cada lugar, qué unidades son apropiadas para cada medición y qué método se usó para obtener el resultado. El marco que sigue se alinea con MISEV 2023 [5] y con las especificaciones estándar de liberación de biológicos de la FDA [25]. Un COA de grado investigación o clínico abordará cada uno de estos parámetros con método, resultado y especificidad de lote.
Figura 4. Los doce parámetros que todo químico verifica antes de aprobar a un proveedor de exosomas. El fallo en cualquiera de estos parámetros debería motivar un seguimiento con el proveedor antes de que el producto entre en un flujo de trabajo clínico.
01 Divulgación de la fuente celular
El COA debe divulgar el tipo de célula productora (MSC, plaqueta, papila dérmica, vegetal u otra), el tejido de origen (médula ósea, tejido adiposo, gelatina de Wharton del cordón umbilical o sangre periférica), los criterios de tamizaje del donante aplicados, el número de pase en el que se recolectaron los exosomas y la composición del medio de cultivo. Las condiciones de cultivo libres de componentes xenogénicos (xeno-free) son preferibles para los productos de grado clínico. Las variables de la fuente afectan directamente la composición de la carga, como establece la literatura proteómica y de microARN [17, 18].
02 y 03 Concentración de partículas y distribución de tamaño por NTA
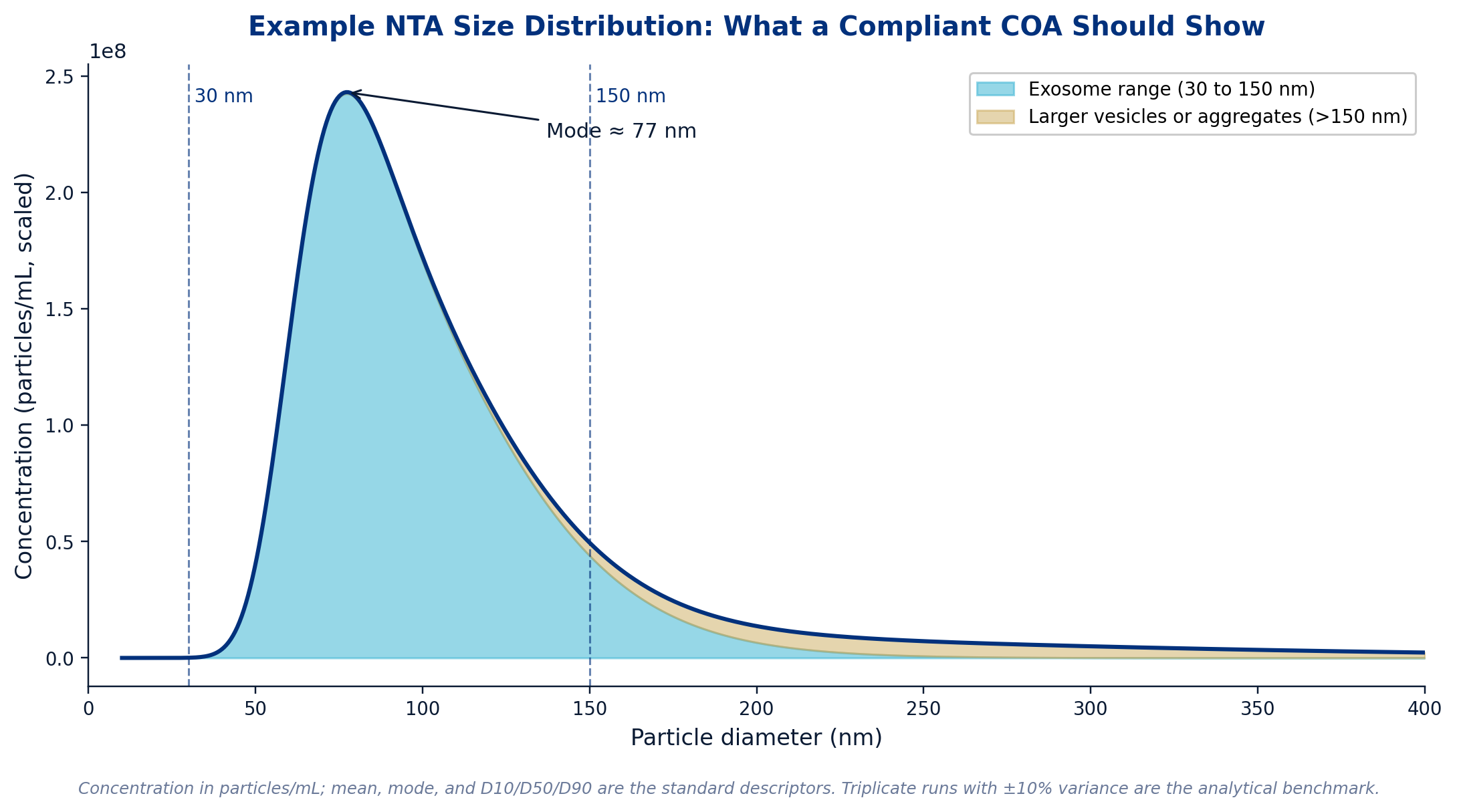
El análisis de seguimiento de nanopartículas (NTA) es el método estándar tanto para la concentración de partículas como para la distribución de tamaño. El COA debe reportar la concentración en partículas por mL, con un rango de trabajo que sitúe la muestra dentro de los límites validados del instrumento (típicamente de 10⁶ a 10¹⁰ partículas por mL para un instrumento de clase Zetaview o NanoSight). La distribución de tamaño debe incluir la media, la moda e, idealmente, los percentiles D10, D50 y D90, con el grueso de la distribución cayendo dentro del rango de exosomas de 30 a 150 nm. Un proveedor de buena reputación proporcionará los datos brutos de NTA, los archivos de video o el histograma, no solo un único número. Corridas por triplicado con una varianza de ±10 % entre réplicas es el punto de referencia analítico para la comparabilidad entre lotes.
Figura 5. Un ejemplo de distribución de tamaño por NTA de una preparación de exosomas conforme. El pico se sitúa dentro del rango de exosomas de 30 a 150 nm, con una cola de vesículas y agregados más grandes que deberían cuantificarse en lugar de ignorarse.
04 Marcadores de superficie positivos
El COA debe reportar al menos tres marcadores positivos del panel MISEV 2023: CD9, CD63 y CD81 son la tríada canónica, opcionalmente complementada con TSG101 o ALIX [5]. La detección debe realizarse por Western blot, citometría de flujo o NTA fluorescente. Una sola tetraspanina reportada de forma aislada no cumple el mínimo de MISEV y debería motivar una solicitud de los marcadores faltantes. Los resultados de marcadores de superficie deben ser como mínimo cualitativos (positivo o negativo), con resultados cuantitativos de porcentaje positivo por citometría de flujo preferibles cuando estén disponibles.
05 Marcadores negativos
MISEV 2023 requiere al menos un marcador negativo para confirmar la baja contaminación por restos celulares. La calnexina, una chaperona del retículo endoplásmico, y GM130, un marcador del cis-Golgi, son los controles negativos más comúnmente reportados [26]. Para las preparaciones derivadas de sangre, las apolipoproteínas A1, A2 y B, más la albúmina, son marcadores negativos apropiados, ya que su presencia indicaría contaminación por proteínas plasmáticas [26]. La presencia combinada de ALIX, CD81 y CD9 junto con la ausencia de albúmina y calnexina confirma el origen endosomal y una alta pureza [26].
06 Esterilidad (USP <71>)
Para cualquier producto destinado a usarse en o cerca de una sala de tratamiento, las pruebas de esterilidad deben seguir la USP <71>, el ensayo estándar de crecimiento aerobio y anaerobio de 14 días [27]. El COA debe reportar “sin crecimiento” y el resultado debe ser específico del lote, no una afirmación general de que la línea de producto ha sido “probada para esterilidad” históricamente. Los proveedores que operan bajo el registro de instalación de externalización 503B cuentan con el marco de esterilidad más riguroso del panorama de compuestos de Estados Unidos.
07 Endotoxina (USP <85> o USP <86>)
Las pruebas de endotoxinas bacterianas son obligatorias para cualquier biológico inyectable o parenteral, y también se recomiendan enfáticamente para las preparaciones tópicas aplicadas sobre piel lesionada o comprometida (posmicroagujas, posláser, pospeeling). Los métodos estándar son el ensayo de Lisado de Amebocitos de Limulus (LAL) según la USP <85> o los métodos de Factor C recombinante (rFC) o de Reactivo en Cascada recombinante (rCR) según la USP <86> [28, 29]. Los resultados deben ser cuantitativos (en EU/mL), con un límite apropiado para la vía de administración. El límite convencional para los parenterales es inferior a 5 EU/kg/h, y la FDA acepta el rFC como una alternativa equivalente cuando la validación del método ha demostrado equivalencia [28].
08 Micoplasma
Los biológicos derivados de cultivo celular conllevan un riesgo real de contaminación por micoplasma proveniente de las células productoras. Las pruebas rutinarias de micoplasma según la EP 2.6.7 (basadas en PCR o en cultivo) deben formar parte del marco de liberación de fabricación [27]. El COA debe reportar un resultado negativo, específico del lote.
09 y 10 ADN residual de la célula huésped y contenido de proteína
El ADN residual de la célula huésped debe cuantificarse, idealmente por debajo de 10 ng por dosis para los productos biológicos, como expectativa estándar de la FDA. El contenido total de proteína (típicamente por ensayo BCA) proporciona el denominador de una métrica de pureza crítica: la relación partícula-proteína. Una relación partícula-proteína alta sugiere una preparación limpia; una relación baja sugiere una contaminación significativa por proteínas no vesiculares provenientes del medio de cultivo o del lisado celular.
11 Almacenamiento y estabilidad
Las preparaciones de exosomas deben almacenarse congeladas, idealmente a menos 80 grados Celsius, y el COA o la documentación adjunta del proveedor debe incluir datos de estabilidad: la cantidad de meses durante los cuales el producto ha sido validado como biológicamente activo en las condiciones de almacenamiento especificadas. La validación de la cadena de frío se extiende a la documentación de envío, con registradores de temperatura preferibles para lotes clínicos de alto valor.
12 Registro de la instalación de fabricación
Las instalaciones de fabricación registradas ante la FDA son verificables a través de la base de datos de registro de establecimientos de la FDA. Para las preparaciones inyectables estériles en Estados Unidos, el registro de instalación de externalización 503B representa el punto de referencia regulatorio actual. ExaVeyra ha cubierto en detalle la distinción práctica entre las farmacias de compuestos 503A y 503B en otro artículo del ExaBlog. Los profesionales que obtienen productos de exosomas para uso clínico deberían confirmar el estado de registro de la instalación de fabricación antes de aprobar a cualquier nuevo proveedor.
MATRIZ DE APLICACIÓN
Distinguir los casos de uso por tipo de práctica
El producto de exosomas adecuado depende de la aplicación, y el mismo marco del COA aplica a los distintos tipos de práctica con diferente énfasis. Un medspa que selecciona un suero tópico posmicroagujas tiene prioridades distintas a las de un consultorio de dermatología que ejecuta un protocolo de restauración capilar, que a su vez tiene prioridades distintas a las de un equipo de ensayo clínico que ejecuta un estudio de Fase 2. La biología y los requisitos de documentación escalan con la aplicación.
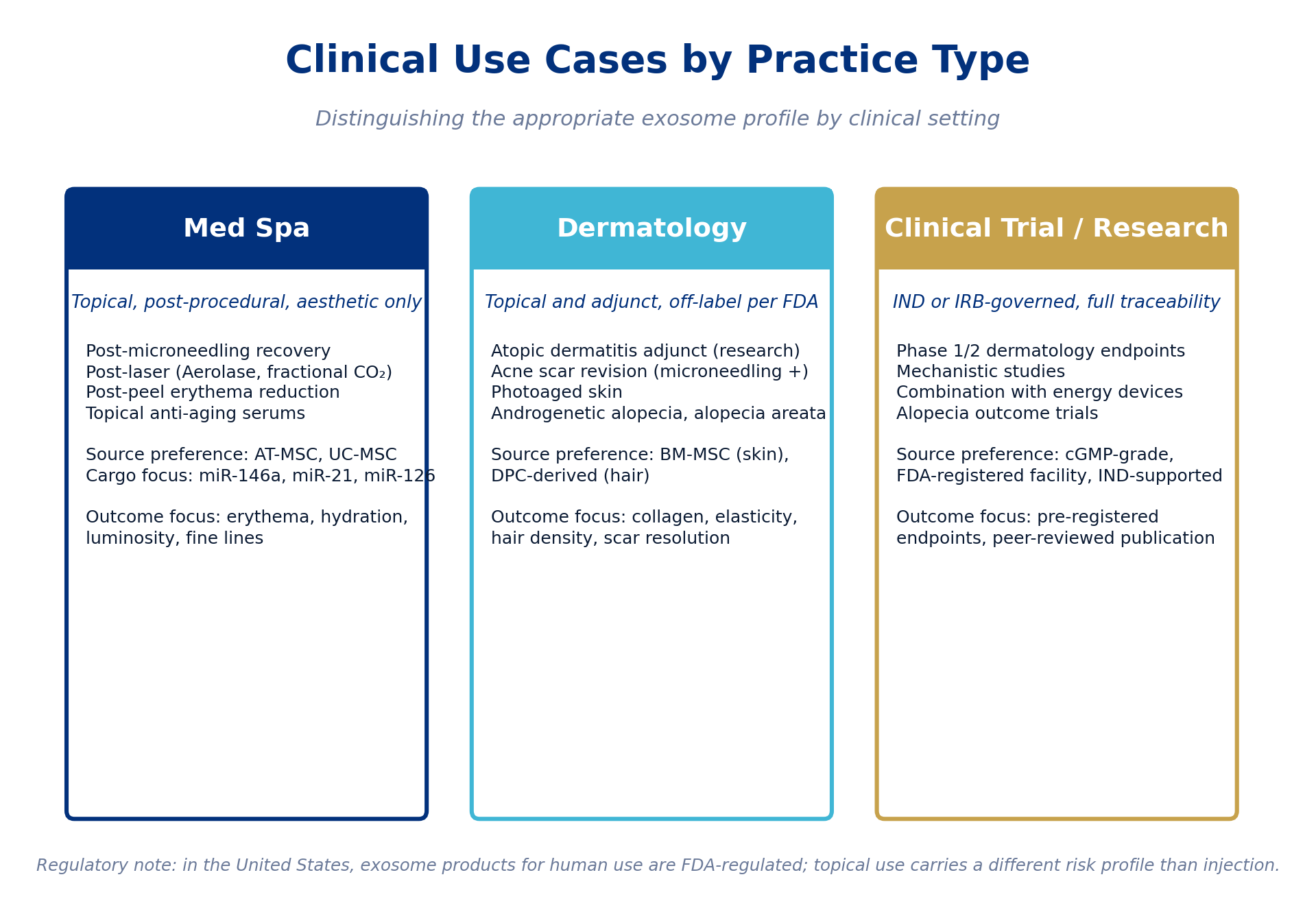
Figura 6. El perfil de exosoma apropiado según el entorno clínico. En Estados Unidos, los productos de exosomas para uso humano están regulados por la FDA, y el uso tópico conlleva un perfil de riesgo distinto al de la inyección.
Medspa: tópico, posprocedimiento, criterios de valoración estéticos
Los medspas que usan exosomas en un flujo de trabajo tópico posprocedimiento (posmicroagujas, posláser, pospeeling, aplicación de suero para investigación en longevidad) suelen beneficiarse de productos de origen AT-MSC o UC-MSC con una señal fuerte de miR-146a, miR-21 y miR-126. Las medidas de resultado relevantes son la reducción del eritema, la hidratación, la luminosidad, la mejora de las líneas finas y la satisfacción reportada por el paciente. La aplicación tópica evita por completo el perfil regulatorio de la vía inyectable y se alinea con la base de evidencia de ensayos clínicos publicados dominante [20, 21, 22].
Dermatología: adyuvante fuera de indicación, restauración capilar, revisión de cicatrices
Los dermatólogos que trabajan fuera de indicación con exosomas suelen enfocarse en indicaciones más específicas: piel fotoenvejecida, adyuvante en dermatitis atópica (solo investigación), revisión de cicatrices de acné en combinación con microagujas, y restauración capilar en alopecia androgenética o areata. Los exosomas de BM-MSC están bien caracterizados para aplicaciones cutáneas [17, 18]. Para la restauración capilar, la señal se concentra en los exosomas derivados de DPC y ASC que portan miR-218-5p y activan Wnt/β-catenina [15, 16, 23]. Las medidas de resultado incluyen la cuantificación de colágeno, la elasticidad, la densidad y el grosor del cabello, la resolución de cicatrices y la satisfacción del paciente.
Ensayo clínico / Investigación: gobernanza IND o IRB, trazabilidad completa
Los investigadores que ejecutan investigación clínica formal con exosomas deberían obtenerlos de instalaciones de fabricación de grado cGMP registradas ante la FDA, con producto respaldado por IND cuando la estructura del ensayo lo requiera. La revisión de 2024 en el Journal of Pharmacology and Pharmacotherapeutics encontró que se han iniciado 90 ensayos clínicos humanos registrados que involucran exosomas hasta 2024, con aumentos constantes año tras año [30]. A principios de 2025, la FDA aprobó su primer IND para un candidato basado en VE [1], y el Ministerio de Seguridad de Alimentos y Medicamentos de Corea aprobó un ensayo de Fase 1b para un producto de VE derivado de MSC de cordón. Para los ensayos, el marco del COA anterior es el piso mínimo; los manuales del investigador, las muestras de retención de lote y la documentación completa de la cadena de custodia son las capas adicionales.
CONTEXTO REGULATORIO
FDA, MISEV 2023 y el piso mínimo de documentación
En Estados Unidos, los productos de exosomas destinados a uso humano están regulados por la FDA. Según el método de fabricación, la composición y el uso previsto, pueden clasificarse bajo la Sección 351 de la Ley de Servicio de Salud Pública como biológicos que requieren una Solicitud de Licencia de Biológicos, bajo el 21 CFR Parte 1271 como células, tejidos y productos basados en células y tejidos humanos si cumplen los criterios de manipulación mínima y uso homólogo, o como medicamentos que requieren revisión de NDA o IND. La FDA ha emitido cartas de advertencia a empresas que hacen afirmaciones terapéuticas no aprobadas sobre productos de exosomas y ha señalado una mayor atención de cumplimiento hacia esta categoría.
MISEV 2023 representa el consenso de la comunidad científica internacional sobre los requisitos mínimos de reporte para los estudios de vesículas extracelulares, y proporciona el piso analítico para cualquier COA comercial que afirme caracterizar exosomas [5, 31]. Un proveedor cuya documentación no aborda el marco MISEV 2023 está, en efecto, pidiendo a los profesionales que acepten la identidad de la vesícula por fe. Ese es el punto de partida equivocado para un producto clínico.
En resumen: el COA es la historia de calidad del proveedor por escrito. Una clínica que sabe qué leer en él tiene una decisión de adquisición defendible. Una clínica que no lo sabe tiene un documento de marketing. La química y las expectativas regulatorias son lo suficientemente claras como para que una práctica clínica pueda exigir a los proveedores un estándar real.
AVISO EDUCATIVO
Este artículo está destinado a profesionales médicos con licencia y tiene únicamente fines informativos y educativos. No constituye consejo médico, orientación sobre protocolos clínicos ni respaldo de producto. Todas las citas hacen referencia a literatura revisada por pares disponible a través de PubMed o de los sitios web de los editores. El estado regulatorio de los productos de exosomas está sujeto a cambios; consulte la guía vigente de la FDA y a asesoría legal calificada.
REFERENCIAS REVISADAS POR PARES
Referencias
[1] Tan F, et al. Clinical applications of stem cell-derived exosomes. Signal Transduction and Targeted Therapy. 2024;9:17. https://www.nature.com/articles/s41392-023-01704-0
[2] Vondrová L, et al. Tetraspanins, More than Markers of Extracellular Vesicles in Reproduction. International Journal of Molecular Sciences. 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC7589920/
[3] Mathieu M, et al. Differential proteomics argues against a general role for CD9, CD81 or CD63 in the sorting of proteins into extracellular vesicles. Journal of Extracellular Vesicles. 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10390663/
[4] Ivanusic D, Denner J. The large extracellular loop is important for recruiting CD63 to exosomes. microPublication Biology. 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10432940/
[5] Welsh JA, et al. Minimal Information for Studies of Extracellular Vesicles (MISEV2023). Journal of Extracellular Vesicles. 2024. https://onlinelibrary.wiley.com/journal/20013078
[6] Fang S, et al. Mesenchymal stem cells-derived exosomal microRNAs contribute to wound inflammation. Science China Life Sciences. 2016. https://link.springer.com/article/10.1007/s11427-016-0240-4
[7] Wang S, et al. Umbilical Cord Mesenchymal Stem Cell-Derived Small Extracellular Vesicles Deliver miR-21 to Promote Corneal Epithelial Wound Healing through PTEN/PI3K/Akt Pathway. Stem Cells International. 2022. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9303509/
[8] Hu Y, et al. Exosomes derived from human umbilical cord blood mesenchymal stem cells stimulate regenerative wound healing via TGF-beta receptor inhibition. Stem Cell Research and Therapy. 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8336384/
[9] He X, et al. Application of mesenchymal stem cell exosomes in the treatment of skin wounds. Burns and Trauma. 2023. https://www.sciencedirect.com/science/article/am/pii/S2590183423000157
[10] Yu Y, et al. Hydrogen Peroxide-Induced Senescence Reduces the Wound Healing-Promoting Effects of Mesenchymal Stem Cell-Derived Exosomes Partially via miR-146a. Aging and Disease. 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7801275/
[11] Wang Y, et al. MiR146a-loaded engineered exosomes released from silk fibroin patch promote diabetic wound healing by targeting IRAK1. Signal Transduction and Targeted Therapy. 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9922687/
[12] Wang S, et al. miR-126 Regulates Angiogenic Signaling and Vascular Integrity. Developmental Cell. 2008;15:261-271. https://www.sciencedirect.com/science/article/pii/S1534580708002876
[13] Zhang L, et al. Exosomes from microRNA-126 overexpressing mesenchymal stem cells promote angiogenesis by targeting the PIK3R2-mediated PI3K/Akt signalling pathway. Journal of Cellular and Molecular Medicine. 2021. https://onlinelibrary.wiley.com/doi/10.1111/jcmm.16192
[14] Pan Q, et al. Exosomes Derived from Mesenchymal Stem Cells Ameliorate Hypoxia/Reoxygenation-Injured ECs via Transferring MicroRNA-126. Stem Cells International. 2019. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6589209/
[15] Hu S, et al. Dermal exosomes containing miR-218-5p promote hair regeneration by regulating beta-catenin signaling. Science Advances. 2020;6:eaba1685. https://www.science.org/doi/10.1126/sciadv.aba1685
[16] Hassanshahi A, et al. Exosomes in trichology: A literature review. World Journal of Stem Cells. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12814429/
[17] Wang ZG, et al. Comprehensive proteomic analysis of exosomes derived from human bone marrow, adipose tissue, and umbilical cord mesenchymal stem cells. Stem Cell Research and Therapy. 2020;11:511. https://pmc.ncbi.nlm.nih.gov/articles/PMC7694919/
[18] Pawitan JA, et al. Differential Wound Healing Capacity of Mesenchymal Stem Cell-Derived Exosomes Originated From Bone Marrow, Adipose Tissue and Umbilical Cord Under Serum and Xeno-Free Condition. Frontiers in Molecular Biosciences. 2020;7:119. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7327117/
[19] Bai S, et al. Proteomics Analyses Reveal Functional Differences between Exosomes of MSCs Derived from The Umbilical Cord and Those Derived from The Adipose Tissue. Iranian Biomedical Journal. 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7944129/
[20] Bai S, et al. Clinical applications of exosomes in cosmetic dermatology. Skin Health and Disease. 2024;4:e348. https://onlinelibrary.wiley.com/doi/full/10.1002/ski2.348
[21] Estupiñan B, Ly K, Goldberg DJ. Adipose Mesenchymal Stem Cell-Derived Exosomes Versus Platelet-Rich Plasma Treatment for Photoaged Facial Skin: An Investigator-Blinded, Split-Face, Non-Inferiority Trial. Journal of Cosmetic Dermatology. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12104007/
[22] Effectiveness of Extracellular Vesicle Application in Skin Aging Treatment and Regeneration: Do We Have Enough Evidence from Clinical Trials? International Journal of Molecular Sciences. 2025;26:2354. https://www.mdpi.com/1422-0067/26/5/2354
[23] Therapeutic potential of stem cell-derived exosomes in hair regeneration: A systematic review. World Journal of Stem Cells. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12305264/
[24] The Innovative and Evolving Landscape of Topical Exosome and Peptide Therapies: A Systematic Review of the Available Literature. Aesthetic Surgery Journal Open Forum. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11023079/
[25] United States Pharmacopeia. USP <71> Sterility Tests. United States Pharmacopeial Convention. https://www.uspnf.com/
[26] Theofilopoulos S, et al. Exosomal Protein Markers as Potential Non-Invasive Biomarkers for Colorectal Cancer. International Journal of Molecular Sciences. 2025. https://www.mdpi.com/1422-0067/26/22/11060
[27] The Critical Role of Quality Control in Exosome-Based Therapeutics: Standards under USP <71>, USP <85>, and ICH Q5A. https://www.atlantisbioscience.com/blog/quality-control-exosome-therapeutics-academic-innovators/
[28] United States Pharmacopeia. USP <85> Bacterial Endotoxins Test. United States Pharmacopeial Convention. https://www.uspnf.com/
[29] United States Pharmacopeia. USP <86> Bacterial Endotoxins Test using Recombinant Reagents. United States Pharmacopeial Convention. https://www.uspnf.com/
[30] Mohan S, et al. Clinical Frontiers of Exosome Research: A Comprehensive Analysis of Human Trials. Journal of Pharmacology and Pharmacotherapeutics. 2025. https://journals.sagepub.com/doi/10.1177/0976500X251361201
[31] Witwer KW, et al. Minimum information for studies of extracellular vesicles 2023: relevance to cell and gene therapies. Cytotherapy. 2024. https://www.isct-cytotherapy.org/article/S1465-3249(24)00727-8/abstract